Sunday is my day to sit and catch up on my casual reading. I look forward to these mornings where I can sit and relax a bit, look into the items on my reading list in Safari that I didn’t have time to get to during the week and check the links posted to Twitter
In that context, I was reading a fascinating article on series of productivity tips from Scott Hanselman, a program manager at Microsoft. This one really caught my attention:
“Conserve Your Keystrokes
“Pulling a page from author and software developer Jon Udell, Hanselman encourages you to ‘conserve your keystrokes.’ What does this mean? He explains by example:
“If Brian emails me a really interesting question about ASP.net … and I send him back an exciting and long, five-paragraph with a code sample email that solves his problem, I just gave him the gift of 10,000 of my keystrokes. But there is a finite number of keystrokes left in my hands before I die, and I am never going to get those keystrokes back and I’ve just gifted them to Brian. And I don’t even know if he reads that email. So what should I do to multiply these keystrokes given that there is a finite number of those keystrokes left in my hands? I write a blog post and I mail him the link. Then after I’m dead, my keystrokes multiple—every time I get a page view that’s 5,000 keystrokes that I did not have to type.”
“‘Keep your emails to 3-4 sentences,’ Hanselman says. ‘Anything longer should be on a blog or wiki or on your product’s documentation, FAQ or knowledge base. ‘Anywhere in the world except email because email is where your keystrokes go to die,’ he says.”
Like most instructors, I spend a lot of time emailing students the answers to questions. Like Hanselman, I actually concluded many years ago that my “keystrokes were dying” and started creating FAQs in my notes to refer students to. Now I realize that I didn’t take it far enough because my keystrokes still die at the end of the course. Not only that, but I find that students often don’t bother to look in the FAQ for their question (it’s not the most user-friendly format).
As a result of all of this, I have created this blog. Here I will post general information, usually for students, that I think people might want to know. Most of this information will be things that I think will be handy not only to the current class but also in future years.
It should be noted that this site is not directly affiliated with Rush University in any way and they are not responsible for the content. Also note well that any ESSENTIAL information for students will be posted to Blackboard – you should not need to check this site to keep up on what’s going on in class.
Having said that, students are welcome to check back occasionally to see if anything new has popped up that, perhaps, they feel would be helpful. Searching for an answer to your question to see if someone else has already asked it (they probably have) would be a pretty good use of this space, as well. With any luck I’ll be able to spend my time posting better answers to questions because I won’t have as many to answer and we’ll all benefit.
Hopefully this will help keep the information alive for years to come instead of dying on a server somewhere in the Triangle Office Building.

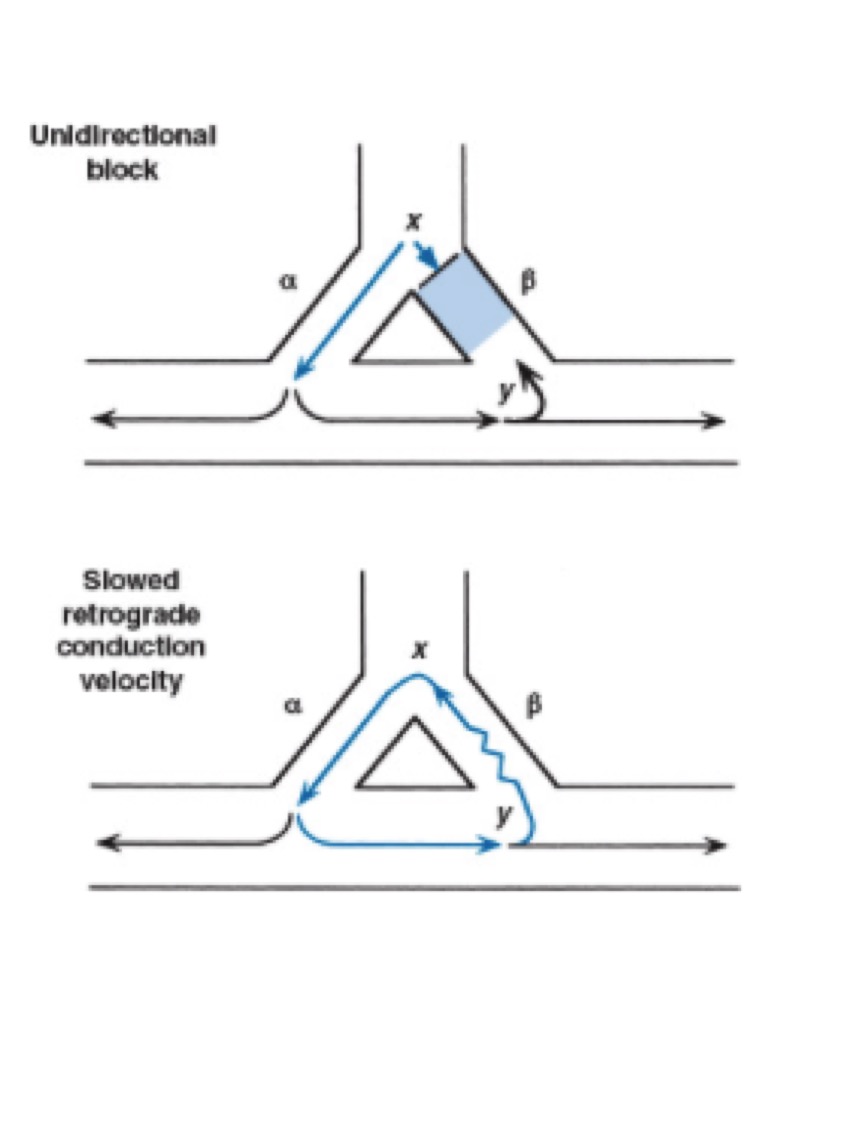 Consider the situation illustrated above. The unidirectional block is in the beta branch of the pathway (top figure). The action potential travels down the alpha branch (which is normal) and back up the beta branch (bottom figure). Note that though conduction is still allowed up the beta branch in a retrograde fashion, these cells are still abnormal and conduction may be slowed (bottom figure, squiggly line). If the action potential goes up the beta branch and reaches the alpha branch after the alpha branch has exited its refractory period, a re-entrant arrhythmia results.
Consider the situation illustrated above. The unidirectional block is in the beta branch of the pathway (top figure). The action potential travels down the alpha branch (which is normal) and back up the beta branch (bottom figure). Note that though conduction is still allowed up the beta branch in a retrograde fashion, these cells are still abnormal and conduction may be slowed (bottom figure, squiggly line). If the action potential goes up the beta branch and reaches the alpha branch after the alpha branch has exited its refractory period, a re-entrant arrhythmia results.
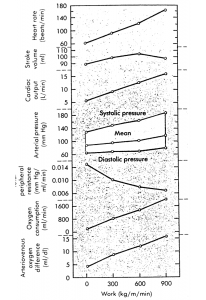 The problem is that, as most of you will recall, in the lecture I did in the Human Simulation Laboratory I said that the MAP wouldn’t change or might decline a little bit with an initial drop followed by a reflexive increase that wouldn’t quite get back up to the starting point.
The problem is that, as most of you will recall, in the lecture I did in the Human Simulation Laboratory I said that the MAP wouldn’t change or might decline a little bit with an initial drop followed by a reflexive increase that wouldn’t quite get back up to the starting point.
 The answer is “b”.
The answer is “b”.